Voluntary vs. Mandatory Bundles
he Centers for Medicare & Medicaid Services (CMS) is the primary payer when it comes to bundlesCommercial bundles are also growing in popularity, though there is high variation in how those are defined and implemented.. The CMS Innovation Center (CMMI) created several programs that focus on bundled care. The bundles fall into two categories: voluntary and mandatory bundles.
Examples of CMS Bundle Programs
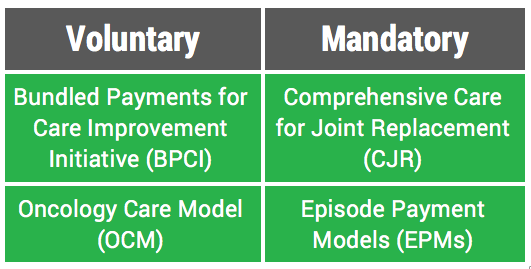
Voluntary Bundles
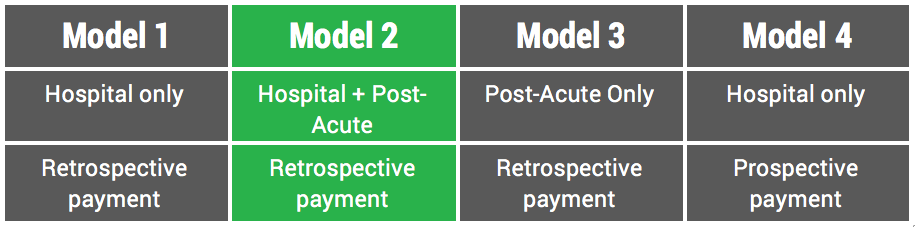
CMS created the voluntary Bundled Payments for Care Improvement Initiative (BPCI) and the Oncology Care Model (OCM) programs to engage care providers in reducing the costs of care for Medicare beneficiaries. BPCI is a bundles “catch-all” with 48 different episodes of care under its umbrella. These range from surgical episodes (e.g., Major Joint Replacement of the (1) Lower or (2) Upper Extremities, separately) to medical episodes (e.g., Nutritional and Metabolic Disorders). It also includes four different “models”There are four timeframes. Each varies in how the awardee, or care-providing entity, receives payment for the costs of patient care. wherein groups ranging from post-acute care practices to integrated delivery systems are responsible for the cost of care for upwards of 90 days. Currently there are 1,343 participants in this model.
The Oncology Care Model focuses on “provid[ing] higher quality, more highly coordinated oncology care at the same or lower cost to Medicare.” The episode of care for these patients spans six-months and there are currently 195 practices engaged in this model.