
Tackle the hard topics: employee schedules
As we started to put together the new discharge team’s schedule, we worried about adding more employees. We looked at all of the daytime teams and wondered if we had the right number of people—could some people float to this new team? We soon realized that we had to address how each team scheduled. Each supervisor had the autonomy to schedule their own teams. While it gave a sense of ownership, it reduced the effectiveness of the overall EVS team. We decided to have one person do central scheduling for everyone so we could cover every team appropriately, every day.
"It was a hard change. Anytime you schedule for 250 people, you’re not going to make them all happy."
It was a hard change. Anytime you schedule for 250 people, you’re not going to make them all happy. Some were worried that the new team would take resources from existing teams. Some senior employees felt they were losing priority scheduling, while junior employees felt better about not having to always work the less-than-prime shifts. We kept emphasizing that the change would not only accommodate patient demand, it would also support the custodian.
Listen to the team
We introduced the changes with a big party and then asked for the team’s input on equipment and supplies. We asked about the other delays they experienced. That’s when we learned about the time-consuming phone calls.
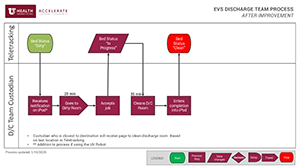
In every discharged room, the custodian had to place a 30-60 second phone call to track the room’s status so the admitting team could then signal the transport team that a room was available. The time spent on the calls added up quickly. We introduced iPads that would provide the same information about room turnaround progress, but with a simple click, saving two to three hours of team time every day.
We also created a centralized stock of equipment that was necessary to clean each room so people wouldn’t have to search for missing supplies, further reducing turnaround times and eliminating waste.