

Learn More:
medical students, Sam and I (Rachel) sensed there was far more to medicine than what is taught in lectures. Later we learned it was the culture surrounding us that molds our professional identity. Called the “hidden curriculum,” this culture can perpetuate both harmful and beneficial systems of thought.
What is the “hidden curriculum” and why should you care?
The “hidden curriculum” is a cultural process in which behavioral modeling via unspoken learning socializes students to what is valued in medical practice.1 It is the accepted stereotypes, hallway conversations, power dynamics and perceptions that comprise our everyday interactions. This informal process overpowers formal curriculum as the “true educator” early in clerkships, and maintains this position throughout a physician’s career.1,2,3 Though it plays a powerful role in the development of our professional identity, students are not typically formally taught how to manage these tacit processes of values, beliefs, expectations and social practices.6
The negative implications to conform to the hidden curriculum can manifest as a loss of empathy, compassion and moral reasoning.1 Historically, this transformation has been regarded as necessary by many educators, who viewed this as 'toughening up' students and preparing them for survival in the medical arena.1, 2, 4, 5
At the University of Utah School of Medicine (UUSOM), we instead found the hidden curriculum to be a neutral tool capable of both negatively and positively influencing students.
Making the hidden curriculum visible: A student-led initiative
In 2018, under the mentorship of Dr. Kathryn Moore, we decided to address the knowledge gap between the formal and hidden curriculum by founding The Core: a student-led group dedicated to providing a medium for cultural knowledge to be passed down from class to class.7 Prior to this, UUSOM strategy for effecting change focused on returning to the humanistic roots of medicine; however, it does not address the practicalities of navigating the hidden curriculum nor how to educate others about its existence.
The Core authors annual guidebooks with fundamental information regarding how to successfully maneuver through the hidden curriculum. Our goal is to equip students with a basic skill set to thrive in the current culture, and to encourage positive deviance from undesirable behaviors. The Medical School Starter Pack for incoming students provides advice and resources from prior classes on how to succeed academically, socially and emotionally in the formal curriculum.
As students transition to clerkships, we offered a workshop about the hidden curriculum as well as the Clerkship Survival Guide which systematically addresses aspects of clerkships, such as performance evaluations, study resources, targeted core rotation advice, plus guidance on rounding etiquette. Currently we are gathering data on the impact these interventions have on student awareness of the hidden curriculum and their ability to navigate it.
A practical tool you can use right now to teach the hidden curriculum
Quick Guide
Download a print copy of the Quick Guide: "The SOLVE Strategy for Teaching Hidden Curriculum" here.
All health care professionals are impacted by the hidden curriculum.4 Therefore, any discipline can benefit from raising awareness of this process. For students in particular, it can ease the transition into the medical profession and may increase physician resilience to burnout.3
The SOLVE strategy, a heuristic approach to problem solving, was adapted for the hidden curriculum and used to teach the UUSOM class of 2022 prior to clerkships to broaden understanding of how culture influences decisions and events.8 It is an excellent tool you and your team can use to create a positive impact in your clinic, operating room, small groups or debriefs.
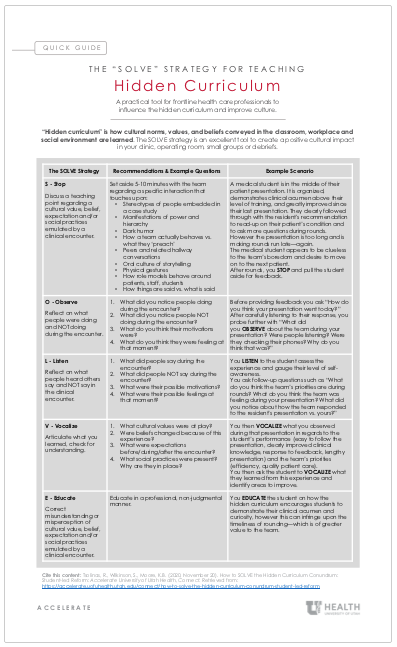
| The SOLVE Strategy | Recommendations & Example Questions |
Example Scenario |
|---|---|---|
|
S - Stop Discuss a teaching point regarding a cultural value, belief, expectation and/or social practices emulated by a clinical encounter. |
Set aside 5-10 minutes with the team regarding a specific interaction that touches upon:
|
A medical student is in the middle of their patient presentation. It is organized, demonstrates clinical acumen above their level of training, and greatly improved since their last presentation. They clearly followed through with the resident's recommendation to read-up on their patient’s condition and to ask more questions during rounds. However the presentation is too long and is making rounds run late—again. The medical student appears to be clueless to the team’s boredom and desire to move on to the next patient. After rounds, you STOP and pull the student aside for feedback. |
|
O - Observe Reflect on what people were doing and NOT doing during the encounter. |
What did you notice people doing during the encounter? What did you notice people NOT doing during the encounter? What do you think their motivations were? What do you think they were feeling at that moment? |
Before providing feedback you ask “How do you think your presentation went today?” After carefully listening to their response, you probe further with “What did you OBSERVE about the team during your presentation? Were people listening? Were they checking their phones? Why do you think that was?” |
|
L - Listen Reflect on what people heard others say and NOT say in the clinical encounter. |
What did people say during the encounter? What did people NOT say during the encounter? What were their possible motivations? What were their possible feelings at that moment? |
You LISTEN to the student assess the experience and gauge their level of self-awareness. You ask follow-up questions such as “What do you think the team’s priorities are during rounds? What do you think the team was feeling during your presentation? What did you notice about how the team responded to the resident’s presentation vs. yours?” |
|
V – Vocalize Articulate what you learned, check for understanding. |
What cultural values were at play? Were beliefs changed because of this experience? What were expectations before/during/after the encounter? What social practices were present? Why are they in place? |
You then VOCALIZE what you observed during that presentation in regards to the student’s performance (easy to follow the presentation, clearly improved clinical knowledge, response to feedback, lengthy presentation) and the team’s priorities (efficiency, quality patient care). You then ask the student to VOCALIZE what they learned from this experience and identify areas to improve. |
|
E - Educate Correct misunderstanding or misperception of cultural value, belief, expectation and/or social practices emulated by a clinical encounter. |
Educate in a professional, non-judgemental manner. | You EDUCATE the student on how the hidden curriculum encourages students to demonstrate their clinical acumen and curiosity, however this can infringe upon the timeliness of rounding—which is of greater value to the team. |
The hidden curriculum is a dynamic influencer of professional identity formation that can simultaneously perpetuate harmful and beneficial systems of thought. This dual utility makes it an excellent target for educational reform. By sensitizing the next generation of physicians to their exposure to it, students will become partners and eventually leaders in a cultural change.
The Core’s interventions, coupled with a broad, multi-level educational commitment to thoughtfully expose the hidden curriculum, can potentially quell current detrimental social norms of medicine and improve physician career longevity.
REFERENCES:
- Bandini J, Mitchell C, Epstein-Peterson ZD, et al. Student and faculty reflections of the hidden curriculum: How does the hidden curriculum shape students’ medical training and professionalization? American Journal of Hospice and Palliative Medicine®. 2017; 34(1): 57-63.
- Martimianakis MAT, Michalec B, Lam J, et al. Humanism, the hidden curriculum, and educational reform: A scoping review and thematic analysis. Academic Medicine. 2015, 90(11): S5-S13.
- Hopkins L, Saciragic L, Kim J, et al. The hidden curriculum: exposing the unintended lessons of medical education. Cureus. 2016; 8(10).
- Ferreira S, Afonso P, & Ramos MDR. Empathy and burnout: A multicentre comparative study between residents and specialists. Journal of evaluation in clinical practice. 2019: 1-7.
- Holmes CL, Harris IB, Schwartz AJ, et al. Harnessing the hidden curriculum: a four-step approach to developing and reinforcing reflective competencies in medical clinical clerkship. Advances in Health Sciences Education. 2015; 20(5): 1355-1370.
- Alsubaie MA. Hidden curriculum as one of current issues of curriculum. Journal of Education and Practice. 2015; 6(33): 125-128.
- Tsolinas, R. & Wilkinson, S. (2020, September 21). Current MD Students Career Development: Other Resources. Retrieved from https://medicine.utah.edu/students/current-students/professional-development/resources/other-resources.php
- Linn, A., & Myles, B. S. (2004). Asperger Syndrome and Six Strategies for Success. Beyond Behavior.
ACKNOWLEDGEMENTS: The authors would like to acknowledge Gina Allyn (Class of 2022), Abigail Luman (Class of 2022), Amanda Cooper (Class of 2023), and Jordan Nishimoto (Class of 2023) as members of The Core and for their contribution to the Medical School Starter Pack and the Clerkship Survival Guide.
Rachel Tsolinas
Samuel Wilkinson
Kathryn B. Moore
Frequent and deliberate practice is critical to attaining procedural competency. Cheryl Yang, pediatric emergency medicine fellow, shares a framework for providing trainees with opportunities to learn, practice, and maintain procedural skills, while ensuring high standards for patient safety.
Hospitalist and Graduate Medical Education director of quality and safety Ryan Murphy explains how Accelerate’s playlists are an infinitely modifiable, curiosity-satiating approach to unifying learners behind a single vision. With more than 15,000 visitors in the last 12 months, it’s worth taking a look.
Empathy is our cognitive ability to understand, communicate, and respond to another person’s perspectives, experiences, and concerns. Pediatrician Diane Liu reflects on the very real challenges of nurturing empathy in the face of the relentless demands of practice.