ess than a decade ago, central-line associated bloodstream infections (CLABSIs) were considered the most pervasive of all hospital-associated illnesses (HAIs). Across the United States, 500,000 patients contracted a CLABSI between 1990-2010—an average of 25,000 per year.
A single CLABSI incident can exact a long-term toll on patients, setting off a cycle of weakened immune system, infection, and possibly septic shock.
CLABSIs’ endemic nature made the path to prevention seem impossibly complex. In 2011, the Center for Disease Control issued an 80-page document listing various techniques to prevent central line infections. Without standardization and simplification, such recommendations were difficult to implement.
In 2011, Utah’s Intermediate Care Unit (IMCU) decided to improve patient safety through a new approach: engage the entire team in identifying and implementing the improvement. Clinical Operations Director Trell Inzunza was an IMCU staff nurse at the time and was chosen to participate on the improvement team.
Here she shares the 4-step process they used to engage the entire team to prevent infection.
THE IMPACT OF CLABSI
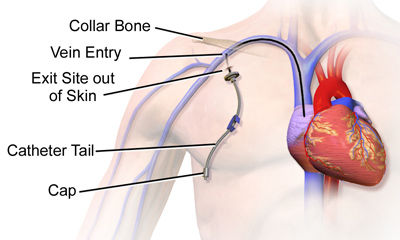
CLABSI are infections that come from central line catheters placed intravenously in the neck, groin, or arm to deliver medication and allow needle-less blood draws. The longer a central line remains, the higher the risk of infection.
CLABSI and other HAIs have a profound impact on patients and US health care. In 2016 alone, over 48,000 HAIs resulted in 3,200 potentially avoidable deaths, contributed over $2 billion in excess costs, added an average of 8 days to the average length of stay.
Ask — How will your next patient be harmed?
Eight years ago, I was a nurse in the Intermediate Care Unit (IMCU). My team was charged with adopting a culture of safety. For us, it started with a question: How will your next patient be harmed?
It was a great question for two reasons. First, it acknowledged that harm happens–it’s inevitable. Second, by using the word “how” it suggested that individuals can do something about it.
Our management team wanted to hear what we had to say so they arranged to have our feedback submitted anonymously. They provided a safe venue which told the team that their feedback was important. As a result, the response rate was higher than expected (greater than 80%).
Listen — To what is spoken (and the silence in between)
The next step was to listen to the answers. Listen to what was spoken and the silence in between.
Feedback pointed to CLABSIs as our next potential harm. While we had only had one infection in the last 12 months, our team believed we could be doing more to prevent CLABSIs.
Learn — Expand your team
As a leader are you providing answers, or are you partnering with your team and resources to find solutions? In IMCU, we had answers. Anyone of us could tell you how infections occurred. What really needed was a solution.
We asked for help and assembled a team of experts from across the University of Utah. Each member of the team brought their own expertise and perspective. It was only possible because we are part of a world class academic hospital!
Our team included many people. Our fearless leader, Carrie Olsen, was steadfast in her mission to keep us on track. Experts from Value Engineering brought lean six sigma principles to help narrow our focus and helped us translate our clinical practice into data and graphs. They helped us understand our problem.
With their help we determined that we needed to create a standard process for our central line care. Infection Prevention introduced us to best practices and helped us understand how rates were calculated and fallouts were attributed. Clinical Staff Education provided exhaustive literature searches and engaging education.
Physician champions challenged our thinking by introducing new perspectives and always made sure we knew our contributions were valued. Our executive sponsor, Dr. Bob Pendleton, at that time brand new to his role, had the best job of all: listen to our concerns and allocate resources.
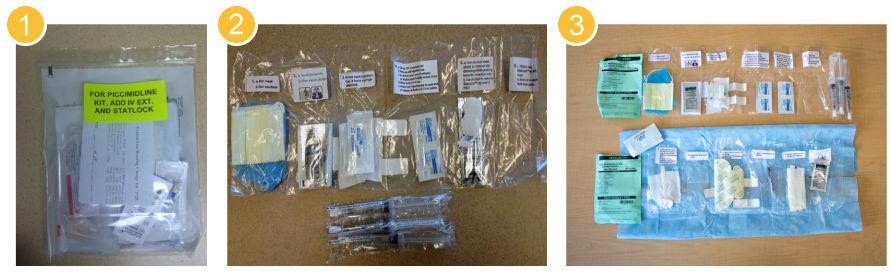
Once we defined our goal to focus on line maintenance we were fortunate enough to be introduced to Dr. Frank Drews , a cognitive psychologist and expert in human factors at the University of Utah. Dr. Drews and his team supported development of central line kits. The kits became our standard process. Importantly, the kits included the exact instruments needed and visual instructions to guide the work while it was happening. Dr. Drews helped to secure grant funding to develop the first prototype and trial the kits.
Original Central Venous Catheter (CVC) Maintenance Kit Concepts
Engage — Step-by-Step Support and Continuous Communication
The next step was to engage. As a leader, are you dedicating time and resources to let staff know that you are interested in their concerns and solutions? Are you finding the time to close the communication loop? We included our team in all stages of the improvement process. Your team wants to know that their voice is being heard.
Learn how U of U Health tackles infection by building strong interdisciplinary teams and utilizing improvement science to create change that sticks.
We found that a critical step in keeping staff engaged was documenting their concerns and communicating follow up during staff meetings. Following up on their concerns and telling them about it was key to maintain and improve staff morale and a feeling of pride in the team’s accomplishment.
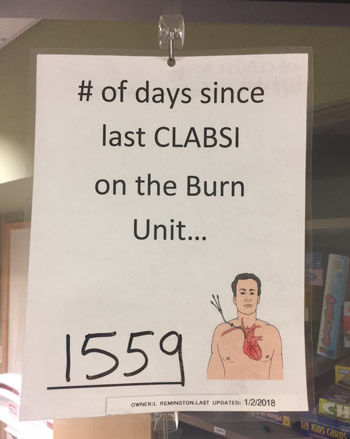
In our work to prevent CLABSIs, we made a point to communicate every win and daily progress to the team. The team was excited, they were proud, and they felt empowered knowing that they had a part in creating a change to improve patient care. Every day, we updated a board that documented how many days it had been since our last CLABSI.
On day 626, we got our first fallout–our first CLABSI infection. We were devastated. We did a root cause analysis and realized that our failure was not the infection. Our failure was not sharing our process with others who were part of our patient’s care team.
Communication is key in team engagement, but it’s also key to success. We kept what we were doing as a pilot on our unit. Our mistake was that we didn’t communicate to the other areas of the hospital that cared for our same patients.
What we took with us was a focus on continuous improvement and safety thinking. The framework to prevent CLABSI led us to other opportunities, some small and some big. Over the next year we reduced our catheter associated urinary tract infection (CAUTI) rates by 45%. Learning together made the work feel impactful and rewarding.
Annotated from Trell Inzunza’s Presentation at the October 31, 2018 Leader Development Institute in Salt Lake City, Utah.
Trell Inzunza
Urogynecology specialist Whitney Hendrickson-Cahill details the steps an interdisciplinary team followed to reduce surgical site infections (SSIs) following hysterectomy procedures, aiming to improve patient outcomes, shorten recovery times, and reduce healthcare costs at University of Utah Health.
Every summer, Utahns head to the mountains for camping, biking, rafting and other activities. And every summer, many a family is left without a stove, or a helmet, or a…because it was left at home. Thrill-seeker and quality manager Cindy Spangler wants to prevent your next packing mishap with a customized camping checklist.
Former Chief Quality Officer Sandi Gulbransen and Accreditation Manager Kemper Funk explain how this umbrella of standards—ISO-9001—relates to our accreditation process and impacts our daily work.