
Learning Objectives
After reading this article, you will be able to:
-
Advocate for timely, transparent, and clear disclosure of medical errors.
-
Identify barriers to disclosure.
-
Use recommended strategies in disclosing errors to patients and families.
Download the 3-page Quick Guide PDF of this article here.
Case Study
Shortly before shift change, a patient with cirrhosis is admitted with spontaneous bacterial peritonitis, a dangerous but treatable abdominal infection. The admitting provider orders the appropriate antibiotic, discusses the case with the hepatology specialist, and signs out care to the evening provider. Shortly thereafter, the hepatologist instructs the evening provider to increase the antibiotic dose. Unfortunately, the new medication order defaults for an administration time the following morning. The evening provider, pharmacist, and nurse caring for the patient all fail to notice the change in timing, and no antibiotics are administered. The following morning, the original provider returns to find the patient considerably worsened and discovers the error.
rrors and unanticipated outcomes are an unfortunate reality in medicine and create significant distress for all involved. Patients report feeling angry, depressed, and traumatized; they lose trust in both their providers and the healthcare system. Providers can feel similar emotions and struggle greatly with how to respond. But how they respond and the timeliness with which they do so has a profound impact on the experience and likelihood of restoring trust.1
What is disclosure?
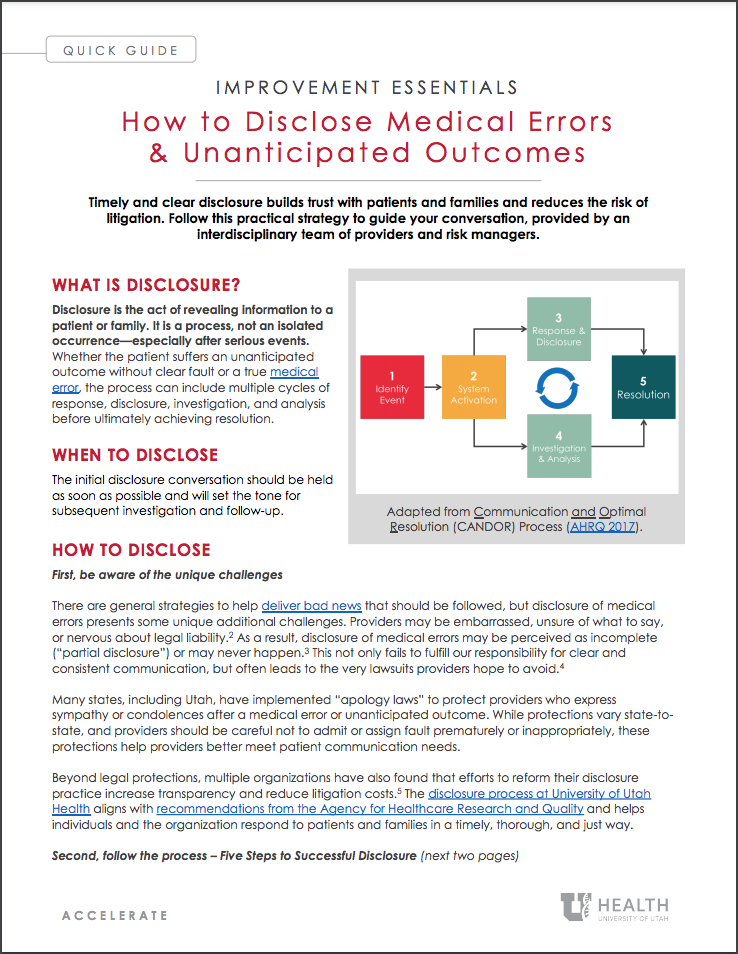
Disclosure is the act of revealing information to a patient or family. It is a process, not an isolated occurrence—especially after serious events. Whether the patient suffers an unanticipated outcome without clear fault or a true medical error, the process can include multiple cycles of response, disclosure, investigation, and analysis before ultimately achieving resolution.
When to disclose an event
The initial disclosure conversation should be held as soon as possible and will set the tone for subsequent investigation and follow-up.
How to disclose an event
First, be aware of the unique challenges
There are general strategies to help deliver bad news that should be followed, but disclosure of medical errors presents some unique additional challenges. Providers may be embarrassed, unsure of what to say, or nervous about legal liability.2 As a result, disclosure of medical errors may be perceived as incomplete (“partial disclosure”) or may never happen.3 This not only fails to fulfill our responsibility for clear and consistent communication, but often leads to the very lawsuits providers hope to avoid.4
Many states, including Utah, have implemented “apology lawsDetails of apology laws vary state-by-state. See more detail about the Utah Health Care Malpractice Act, Utah Rules of Evidence, and relevant case law.” to protect providers who express sympathy or condolences after a medical error or unanticipated outcome. While protections vary state-to-state, and providers should be careful not to admit or assign fault prematurely or inappropriately, these protections help providers better meet patient communication needs.
Beyond legal protections, multiple organizations have also found that efforts to reform their disclosure practice increase transparency and reduce litigation costs.5 The disclosure process at University of Utah Health aligns with recommendations from the Agency for Healthcare Research and Quality and helps individuals and the organization respond to patients and families in a timely, thorough, and just way.
Second, follow a process: Five Steps to Successful Disclosure
The following Five Steps to Successful Disclosure are recommended for the initial disclosure meeting after a medical error or unanticipated outcome.
Step 1: SET UP the conversation
Don’t wait! Do this as soon as possible after the event is discovered.
Organize. Gather as much information as possible for the patient and family. Consider which members of the patient’s personal support system should be present. Identify which members of the health care team should take part in the disclosure with you. The attending provider should be present if possible, but you may not be able to wait.
Set the stage. Find a private and quiet place to meet. Know and use the patient’s name. Introduce yourself and any other individuals in attendance. Sit down. Minimize distractions.
Make an opening statement. Start from the beginning and prepare the patient/family with a shot across the bow: “There has been an unanticipated event in your care and I am here to tell you everything I can.”
Share the information you know. Explain objectively what occurred: “You did not receive the antibiotics we intended to give you last night.” Make factual conclusions and resist the urge to speculate on what may have happened.
Step 2: LISTEN and assess understanding
Listen – allow silence, explore emotion. After sharing a sentence or two about the event, ask if they are ready to hear more details. Allow time for a response. Throughout this conversation, there may be comments or behaviors reflecting grief responses such as anger or disbelief.
Assess understanding. Depending on the situation, patients and families may misinterpret or not hear information discussed. Be ready to repeat information or give information in another way if needed. Encourage patients and families to ask questions so they gain understanding. Anticipate varied responses from different people. Be prepared to listen and offer support.
Step 3: APOLOGIZE sincerely
Allow yourself to be vulnerable. Vulnerability is sincerity—it’s okay to feel uncomfortable. You should offer words of apology and condolences such as, “I am sorry this happened.” Apologize more than once. When appropriate, use phrases of reassurance such as, “We are going to take care of you.”
Avoid blame. Be careful not to prematurely assign blame with phrases like “we screwed up,” or “this is _____’s fault.” Subsequent conversations after additional investigation will better address this.
Step 4: DISCUSS next steps
Console. You can promise patients will receive the ongoing medical care they need. “We will monitor you closely and provide any further care you need.”
Introduce investigation and what to expect. If certain details remain unclear, explain that further investigation will take place. You can assure the patient that results of this investigation will be shared with them and inform specific actions to prevent a similar event from happening again.
Provide a contact. Identify a contact for patients and families who will manage follow-up communication to discuss the situation. Be as specific as possible.
Step 5: SUPPORT the patient/family, yourself, and your team
Spiritual and emotional support. Consider inviting a behavioral health provider or clergy to the meeting. Otherwise, offer to facilitate services afterwards.
Financial support. If finances are raised as a concern, acknowledge that as a legitimate concern and explain that this will be addressed by the organization. The patient and family will receive specific and separate follow up about finances.
If a patient dies unexpectedly, be sure to use the word “dead”, “died”, or “death” to be clear about what you are saying. Use the patient’s name.
Death of a patient is a significant event and will result in numerous coordinated actions from members of the healthcare team. Familiarize yourself with the process, leverage support services, and take your time to walk family through the next steps.
Recognize the impact medical errors, especially those resulting in death, will have on you and your team. Health care providers can become the “second victim” of medical error. Be proactive about seeking support from local resources like the Resiliency Center.
Contact Risk Management for any general assistance with disclosure or after any serious unanticipated outcome.
Conclusion
Let's return to our patient with cirrhosis. From the moment the error was discovered, immediate actions were taken to care for the patient and disclose the event to the patient’s family. A report was filed in the organization’s event reporting system, and further investigation identified the various failures that allowed the error to lead to harm. The patient unfortunately suffered complications from her abdominal infection and passed away in the hospital. A formal interprofessional review identified strategies to reduce the risk of a similar event in the future. The patient’s family was deeply saddened, but was regularly updated and included throughout the entire process.
Additional Learning
Read the University of Utah Health complete Disclosure Guideline.
Watch the introductory video on “Disclosing Error” from as part of the UACT training series.
References
-
Gallagher TH, Waterman AD, Ebers AG, Fraser VJ, Levinson W. Patients’ and Physicians’ Attitudes Regarding the Disclosure of Medical Errors. J Am Med Assoc. 2003;289(8):1001-1007.
-
Mcdonnell WM, Guenther E. Narrative Review: Do State Laws Make It Easier to Say “I’m Sorry?” Ann Intern Med. 2008:811-816.
-
Gallagher TH, Garbutt JM, Waterman AD, et al. Choosing Your Words Carefully. Arch Intern Med. 2006;166(15):1585. doi:10.1001/archinte.166.15.1585
-
Vincent C, Young M, Phillips A. Why do people sue doctors ? A study of patients and relatives. Lancet. 1994;343(8913):1609-1613.
-
Mello MM, Studdert DM, Kachalia A. The medical liability climate and prospects for reform. JAMA - J Am Med Assoc. 2014;312(20):2146-2155. doi:10.1001/jama.2014.10705
Ryan Murphy
Suzette Goucher
Carrie Sullivan
Amanda Moloney-Johns
Christina Derbidge
Jared Henricksen
Health care is full of high emotion—especially right now. Thankfully, there’s a simple framework we can follow to de-escalate with compassion. Hospitalist and UACT co-director Claire Ciarkowski introduces NURSE: a simple mnemonic for responding with empathy.
In Ghana, Value Engineer Cindy Spangler, surgeons Kate Smiley and Marta McCrum found that patient safety rests on simple ideas that are hard in practice.
Feedback is often an area that breaks down under the rigors and pressure of clinical activity. Clinician educators Pete Hannon and Kathleen Timme introduce a methodology that can provide insight, inspire goal setting, and help improve clinical performance.